Frontal Subcortical Circuits
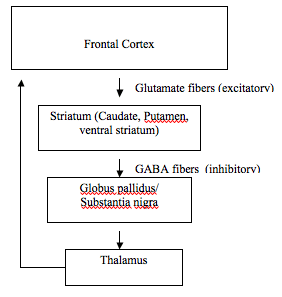 The General structure shared by ALL frontal-subcortical circuits (direct connections) (CSGT: Cortex, Striatum, Globus Pallidus, Thalmus)
The General structure shared by ALL frontal-subcortical circuits (direct connections) (CSGT: Cortex, Striatum, Globus Pallidus, Thalmus)
There are 5 frontal-subcortical circuits that provide a neuroanatomical basis for movement and behavior, named by either function or cortical site of origin.
- Each circuit uses the same transmitters at each anatomic site.
- The relative anatomic positions of the circuits are preserved in each circuit structure (i.e., dorslateral PFC projects to dorslateral region of the caudate).
The 1st two circuits are motor:
Motor (Supplementary Area-Subcortical) Circuit
General control of preparatory premovement activity and serial/parallel processing of movements initiated in the cortex: somatomotor system governing movement of limb and body in space.
Oculomotor (Frontal eye fields-subcortical) Circuit
Visuomotor system for orienting the head and eyes to the environment.
The other three are more behaviorally related, each with signature neurobehavioral clinical syndromes.
The Dorsolateral Circuit
Damage typically results in Executive Dysfunction including:
- poor organizational strategies,
- poor memory search strategies,
- Stimulus-bound behavior/environmental dependency,
- impaired set shifting & maintenance,
- verbal-manual dissociation.
 Figure A: Origin of the Dorsolateral Curcuit.
Figure A: Origin of the Dorsolateral Curcuit.
Orbitofrontal Circuit
Has two parallel subcircuits Lateral & Medial. Personality Change is the hallmark of orbitofrontal dysfunction, including:
- irritability,
- lability,
- fatuous euphoria,
- inappropriate response to social cues,
- undue familiarity,
- lack of empathy.
- These pts. often perform normally on the WCST.
- Acquired OCD may result from OF lesions.
 Figure B: Origin of the Orbitofrontal circuit (Lateral in green, medial in red & blue).
Figure B: Origin of the Orbitofrontal circuit (Lateral in green, medial in red & blue).
The Anterior Cingulate circuit
Mediates motivated behavior, thus damage to this circuit results in an apathetic syndrome. Bilateral lesions often results in akinetic mutism. Other symptoms may include,
- psychic emptiness,
- poverty of spontaneous speech,
- indifference to pain,
- poor response inhibition,
- reduced creative thought.
 Figure C: Origin of the Anterior circuit
Figure C: Origin of the Anterior circuit
Direct and Indirect Pathways
Each direct circuit is modulated by an indirect pathway
 The direct and indirect frontal subcortical loops (red = excitatory connections; blue = inhibitory connections).
The direct and indirect frontal subcortical loops (red = excitatory connections; blue = inhibitory connections).
- Excitatory glutaminergic corticostriatal fibers
- Direct loop’s inhibitory GABA/substance P fibers (associated with D1 receptors) from the striatum to the globus pallidus interna/substantia nigra pars reticulata
- Indirect loop’s inhibitory GABA/enkephalin fibers (associated with D2 receptors) from the striatum to the globus pallidus externa
- Indirect loop’s inhibitory GABA fibers from the globus pallidus externa to the subthalamic nucleus
- Indirect loop’s excitatory glutaminergic fibers from the subthalamic nucleus to the globus pallidus interna/substantia nigra pars reticulata
- Basal ganglia inhibitory outflow via GABA fibers from the globus pallidus interna/substantia nigra pars reticulata to specific thalamic sites.
- Thalamic excitatory fibers returning to cortex (shown in contralateral hemisphere for convenience).
The Direct connection Disinhibits the thalamus. The Indirect connection Inhibits the thalamus.
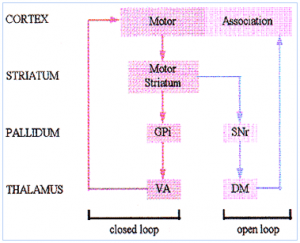
Open and closed loops
Although each of the 5 circuits comprises a closed loop, there are also open elements in each circuit. This allows for posterior association cortices to affect frontally mediated behavior or to serve as communiction points between the three circuits.
The numerous structures and the many transmitters, receptors, and modulators involved in these circuits account for the observation that lesions in different brain regions may have similar behavioral effects.